
You've completed hormone injections and egg retrieval. Now, your clinic calls: they recommend a day 5 rather than a day 3 transfer. What is a blastocyst? Why wait? Does this improve your chances?
To help you understand your options, let's break down what blastocyst stage embryo transfer involves and explain why this approach may offer certain advantages for your IVF journey.

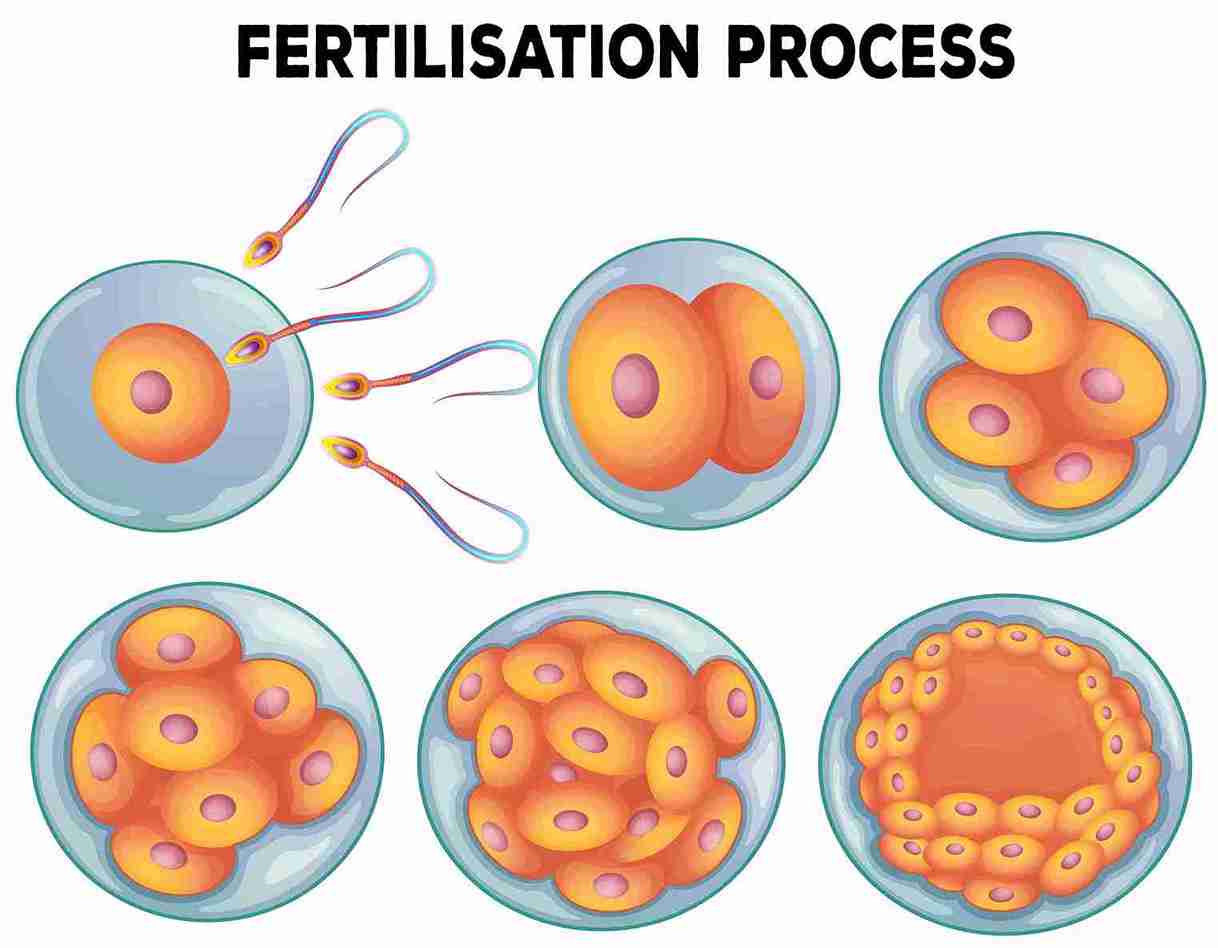
A blastocyst is a 5-6-day-old embryo. After fertilisation, the egg divides: two cells on day 1, 6-8 cells by day 3, and around 100-200 cells by day 5 or 6—now a blastocyst.
At this stage, the embryo looks completely different under a microscope. It has:
The blastocyst is when the embryo gets ready to implant in your uterus.
Blastocyst IVF follows the same steps as regular IVF but differs in the timing of the transfer.
Here is how it works:

Why wait longer? Why not transfer on day 3? There are solid benefits of blastocyst transfer.
Many embryos look good on day 3 but stop growing by day 5. Letting them develop longer reveals which are strong enough for pregnancy. About half of the day-3 embryos don't reach the blastocyst stage. This means transfers aren't wasted on embryos unlikely to result in a pregnancy.
Studies show blastocyst transfer has higher pregnancy rates than day-3 transfer, especially if you're under 35. Rates can be 20 percentage points higher because blastocysts are more developed and ready for implantation. The uterus is also more receptive at this stage.
In the past, doctors transferred 3–4 day-3 embryos to increase chances, sometimes causing multiple pregnancies. With blastocysts, only one embryo is usually transferred, increasing the chance of pregnancy and lowering the risk of multiples.
For genetic testing, blastocysts are preferred. Cells can be removed from the trophectoderm without harming the inner cell mass, allowing for more accurate chromosome analysis.
Naturally, embryos enter the uterus as blastocysts on day 5. Transferring a blastocyst syncs the embryo and uterus.
The main difference is timing and embryo selection.
Cleavage Stage (Day 2-3) Transfer:
Blastocyst (Day 5-6) Transfer:
Day-3 transfer is like betting on horses before a race. Blastocyst transfer lets you bet after seeing which ones can run.
Understanding the differences, you might wonder if blastocyst transfer is right for you. Here’s who may benefit most and why it’s not ideal for everyone.
Blastocyst transfer is most beneficial for women under 35, those with multiple good-quality embryos, couples who have had failed IVF cycles, people who wish to avoid twins by opting for single embryo transfer, and women with good ovarian reserve. On the other hand, your doctor may suggest a Day-3 transfer if you have very few embryos (typically less than 4), if this is your first IVF cycle, if your previous cycles showed poor embryo development in culture, or if you are older with poor embryo quality.
The main worry is that not all embryos reach the blastocyst stage. For example, 6 embryos on day 3 may yield only 2–3 blastocysts, or rarely none, leading to cancelled transfers. However, those embryos likely would not have worked even if transferred earlier.
Growing embryos to day 5 requires excellent lab conditions. Not all clinics have this. Choose a clinic with strong blastocyst success rates.
Some clinics charge extra for extended culture. Ask about costs upfront.
You may also wonder whether frozen embryos can be used for blastocyst transfer and how their results compare with those of fresh transfers.
Yes. Frozen blastocyst transfer works well. Many IVF clinics freeze all blastocysts and transfer them in a later cycle, when your body has recovered from retrieval. Success rates for frozen transfers are similar to, or even better than, those for fresh transfers, since the uterus is not affected by stimulation. Frozen embryos stay viable for over 10 years.
Success rates depend on age and clinic quality. If you are under 35, there is a 50-60% pregnancy rate per blastocyst transfer. It reduces to 40-50% if you are 35-40, and reduces further to 20-35% when you are over 40. These are averages; your individual chances depend on egg and sperm quality, uterine health, and the clinic's expertise.
Blastocyst transfer isn't magic, but it's a smarter IVF approach. You transfer embryos that have been proven to develop, not just hope. While embryos may not reach day 5, it's better to know now than waste a transfer. If you have several good embryos and a high-quality clinic, blastocyst transfer offers the best chance of pregnancy and lowers twin risk. Discuss with your doctor if it's right for you.

The main risk is that embryos might not develop to the blastocyst stage, leaving no embryos to transfer. This happens in about 10-20% of cases, more often in older women or with poor-quality embryos. The good news? Those embryos likely would not have resulted in a pregnancy even if they had been transferred earlier. Other small risks are the same as regular IVF, like infection, bleeding, or ovarian hyperstimulation syndrome. Blastocyst transfer itself does not add medical risks to you.
Yes, frozen blastocyst transfer is common and works well. Success rates are comparable to, or sometimes better than, fresh transfers because your body can recover after egg retrieval. Frozen blastocysts stay viable for over 10 years. Many IVF clinics in India now freeze all blastocysts and transfer later when your uterus is more receptive. This "freeze-all" approach is becoming standard.
Yes. Blastocyst transfer usually gives higher pregnancy rates than day-3 transfers, especially for women under 35. Rates may be about 20 percentage points higher since only the strongest embryos reach this stage. Matching natural implantation timing also helps. However, it requires enough embryos to reach the blastocyst stage. Speak to your doctor.
For most couples, yes. Blastocyst transfer lets doctors select the strongest embryos, offers higher pregnancy rates per embryo, and allows you to transfer fewer embryos, reducing twin risk. However, it is not right for everyone. If you have very few embryos, fewer than 4, a day-3 transfer might be better; you do not want all embryos to stop before day 5. Women over 38 with poor embryo quality might also do better with earlier transfer. Your clinic's lab quality matters too. A good clinic will recommend what is best for your situation.

















